Study tests effectiveness of mixed reality in neurosurgery.
Placing an external ventricular drain (EVD) is a routine but high-stakes neurosurgical procedure used to relieve intracranial pressure. It’s typically done in emergency settings — and often performed freehand, without real-time imaging.
The surgeon identifies an anatomical point on the skull and inserts a catheter into the brain’s ventricles to drain cerebrospinal fluid.
The problem? Up to 60% of these insertions are inaccurate, leading to ineffective drainage and increased risk of complications or repeated procedures. While neuronavigation systems can improve accuracy, they are costly, time-consuming to set up, and not always available in emergencies.
To address this challenge, researchers from the University of Bologna developed NeuroMix, a mixed reality (MR) simulator for EVD placement training. The goal: help trainees build procedural accuracy that remains strong even without digital assistance.
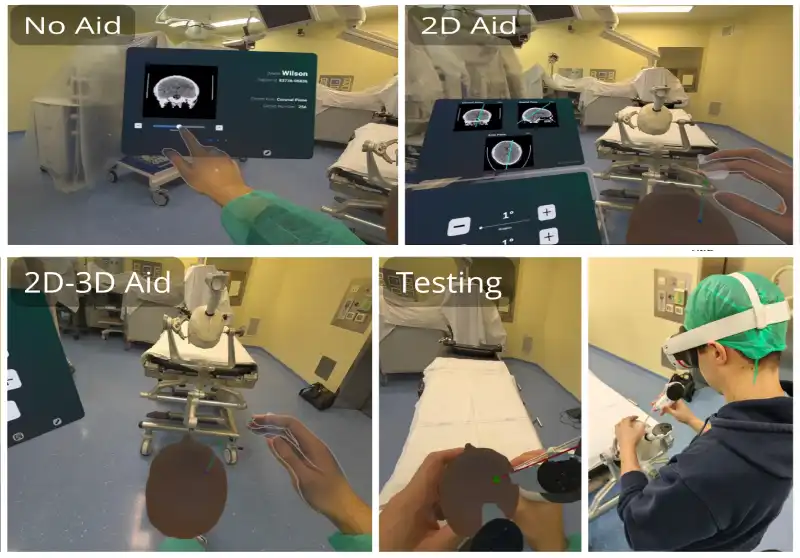
The study compared three training conditions:
- No Aid (only traditional CT scan images),
- 2D Aid (CT images with projected catheter trajectory),
- 2D–3D Aid (adds animated 3D guidance).
After virtual training using the Meta Quest 3 headset, all participants completed a real-life test using a physical catheter and skull model, without any MR-based visual guidance.

Participants trained with the combined 2D–3D visual aid performed best in the physical test:
- Average error was just 1.47 cm, compared to 2.64 cm in the untrained control group.
- This represents a 44.3% improvement in accuracy.
- These participants also had lower tilt and rotation angle errors.
Even without guidance during the real-world test, the group that had immersive training retained better spatial understanding, suggesting that mixed reality helped reinforce memory of the correct angles and depth.
Although more accurate, the trained groups were slower than the control group during the test phase:
- Participants using visual aids took longer during training (up to 138 seconds vs. 62 seconds with no aid).
- In the test phase, they still spent more time — a likely sign of deliberate and cautious execution.
The study notes that training focused entirely on accuracy, with no emphasis on speed, which explains the trade-off.
All training versions received high usability and acceptance scores, even among participants with no prior experience using mixed reality. The 2D–3D interface, despite offering more visual information, did not increase mental workload
The interface design drew inspiration from existing clinical navigation software, which helped reduce cognitive friction and made the learning experience more intuitive.
NeuroMix was built with Unity and the Meta Quest 3, offering a portable and cost-effective solution.
Unlike neuronavigation tools used in surgery, NeuroMix isn’t meant for intraoperative use. Instead, it gives medical professionals a safe, controlled way to train — and retain — essential skills, especially for procedures where high error rates still persist.
📘 Reference: Cascarano, P., Loretti, A., Martinoni, M., Zanuttini, L., Di Pasquale, A., & Marfia, G. (2025). Towards the target and not beyond: 2D vs 3D visual aids in MR-based neurosurgical simulation (arXiv:2506.05164v1). arXiv.